I: Target:
This summary is designed for the patient who has or may have lipedema and is considering surgical treatment. It is also directed to healthcare professionals who encounter women with lipedema.
Overview: Lipedema can be confusing, misdiagnosed, disabling and psychologically demoralizing. Lipedema is common (probably at least 10% of the female population). It is often confused with obesity, lymphedema and chronic venous disease. We know that lipedema is a progressive inflammatory disease; symptoms stem from increased extracellular fluid and abnormal fat nodules in the subcutaneous tissue.

Diagnosis: Hallmark signs of lipedema are bilateral disproportionate fat deposits in the extremities; sensitivity to touch or pain and increased risk of bruising in affected areas. There is often a positive family history.
Hormonal changes (puberty, pregnancy, menopause) often exacerbate disease. And standard weight reduction programs, even bariatric surgery is ineffective. (Appx 1: Diagnosis, stage and type)
Impact of Lipedema: Lipedema, even in early stage, can cause decreased mobility, impair quality of life and work. There is physical, psychological and functional impairment. Lipedema can progress to greater loss of mobility and function and impair joints leading to total joint replacement.
Is lipedema a disease of Lymph tissue? No. Normally, the body manages extracellular fluid through lymphatic drainage. Lipedema is a progressive inflammatory process: 1. There is more fluid build-up than normal drainage (lymph) can handle and 2. there is growth of subcutaneous fat nodules that block lymphatic drainage. Pain, tenderness to touch, bruising and heaviness that are common to almost all women are the result of this inflammatory fluid overload. Surgical treatment can improve lymphatic flow.
Initial treatment for lipedema: The first line of treatment for lipedema is: 1. controlling inflammation with dietary and lifestyle changes: anti-inflammatory diet, aquatic physical exercise, manual lymphatic drainage and antioxidant herbal medicines; and 2. managing extremity swelling with complex decompressive therapy (CDT): 1. medical grade knitted compression garments, Lymph-Press or pneumatic compression devices and manual lymphatic drainage ( MLD) – a specialized massage where lymph fluid is physically massaged to the groin.
Limitations of conservative therapy: Which patient benefits from conservative, non-surgical therapy and for how long is unknown. Decompressive treatment can improve symptoms. This report of 5 cases, different stages of lipedema showed an improvement in symptoms, quality of life using the QuASiL (validated lipedema questionnaire) and measurement of limb volume. All patients followed the anti-inflammatory lifestyle regimen. The authors conclusion: “Treatment objectives can be different for each patient. Non-surgical treatment of lipedema is feasible in selected cases.” (Amato 2021). Despite the lack of a large clinical study of non-surgical treatment for lipedema, the current insurance guideline requires all patients to have documented “no response to at least 3 months of conservative management” (BCBS 2023).
Why consider surgical treatment of lipedema: Surgical treatment of lipedema is the only treatment that removes the abnormal lipedema fat and slows the progression of disease. Using liposuction technologies for lipedema reduction surgery has been consistently shown to 1. decrease pain and sensitivity in the legs, 2. improve functional abilities like walking, working, exercising and 3. prevent long term progression of the disease.
Risks of Surgical treatment: The goal of surgical treatment is to remove the inflammatory lipedema fat and fluid while preserving or restoring lymphatic function. Liposuction, or the extraction of fat with long, thin cannulas has been modified for lipedema surgery: Only axial treatment (in the direction of the limb), awareness of major lymphatic vessels, avoidance of fluid overdistention, and gentle technique with power (vibratory) or water (water jet pulse) is recommended. Damage to the subdermal blood supply, trauma to lymph channels or later stage of disease can lead to secondary lymphedema even 6-12 months after the procedure.
Current controversy in treatment: Ideally, to know whether one treatment or another is best, assuming they are both likely to produce a positive outcome, a randomized study is performed. With lipedema, the treatment options of decompressive therapy and surgical debulking are both effective treatments, though not equivalent. One is used initially, the other when the first has failed. While there may be benefit from decompressive therapy, there is no study demonstrating the predicted duration of benefit or ability to delay disease progression. In the last eight years there are eight peer-reviewed studies of women treated with surgical lipedema care, evaluated with validated questionnaires statistically analyzed, that show unequivocal benefit from lipedema reduction surgery. (Wright (2023), Herbst (2021), Bauer (2019), Buck (2016), Kruppa (2022, Witte (2020), Baumgartner(2020), Dadras (2017))* As complimentary treatments for a heterogeneous population of patients (different stages of disease), it is difficult, possibly unethical, to withhold surgical care for a woman who is likely to experience a significant improvement in quality of life and function.
Insurance position: Major insurers in the United States have failed to embrace lipedema as a progressive chronic disease effectively treated by surgical care.^ There are no CPT codes for lipedema reduction surgery; liposuction codes (15877-15879) are placeholders for cosmetic non-reimbursable procedures. Lipedema is often not recognized, confused with obesity and even for doctors not really understood. Despite overwhelming evidence to the contrary, one major insurance carrier has questioned the benefit of surgical care, “the reliability of reported outcomes is uncertain and durability of the procedure (surgical treatment of lipedema) is unknown.” (BCBS 2023). In 2024, best care is determined by evidence based medicine (peer-reviewed studies) and expert consensus conferences. Both of which have been discounted by current insurance recommendations.
Are there lipedema studies with “validated questionnaires” that show the benefit of surgical treatment for lipedema? Yes. There are 9 published peer-reviewed studies from 2017 to 2023** demonstrating the effectiveness of surgical treatment for lipedema. These studies showed (with statistical significance) that after lipedema reduction surgery patients experienced:
- A significant reduction in pain, sensitivity to touch and discomfort
- 89% women had preop pain and 86% had a reduction in pain after surgery
- A reduction in bruising and swelling
- 36% stated swelling resolved after LRS and 30% were able to stop using compression garments within 3 months.
- 90% reported bruising preop which decreased to 43% after surgery
- Improvement in mobility and walking
- 81% reported impaired walking due to knee (72%), thigh(62%), leg pain(60%) or knee arthritis(41%). In every stage of disease walking improved: Stage 3: (96%), Stage 2: (88%), Stage 1:(33%). 82% of women returned to their activities within one month.
- Early surgical treatment (Stage 1 and 2) has more profound benefit, limiting the progression of disease.
- Stage 2 and 3 patients were followed for up to 2 years. All patients improved but the results were more profound for Stage 2 patients
- Focusing on early stage disease (Stage 1 and 2): the need for manual lymphatic drainage dropped after surgery from 89 to 40% and the need for compression garments dropped from 95% to 32%.
- Lymph-sparing lipedema reduction surgery removes a large volume of abnormal fat.
- After lipedema fat removal, lymphatic flow in the legs can return to normal
- Mean lipedema tissue reduction was frequently 10-12lb per procedure with a mean total reduction over 1-4 procedures of 28.4lb.
- These large volumes are very different than cosmetic liposuction for appearance only.
- Knee kinematics (clinical measurements) demonstrated improvements in movement, knee mechanics and quality of life equivalent or better than published data for total knee replacement.
II:**Referenced Evidenced-based Studies:
Wright (2023): Lipedema Reduction Surgery Improves Pain, Mobility, Physical Function and Quality of Life: Case series report
Case report: 189 consecutive patients (507 procedures) BMI: 34 =/- 7.5 Age: 51+/- 11.5 Country: (USA) Stage: 96% Stage 2 and 3LRS technique: Preop mapping of veins and lymphatics; PAL, removed avg 5 liters per patient per session, avg 4 sessions. Follow-up: up to 4 years. Evaluation: Validated questionnaire for function and QOL: PROMIS and RAND short form-36. Also clinical knee kinematics and Bioimpedance analysis. Impact: after Lipedema reduction surgery.: Demonstrated significant improvement in mobility, knee ROM, gait, QOL, social function and pain for all stages. ( similar to findings from Germany, Spain, UK); Improvements in movement, knee mechanics, QOL equivalent or better than published data for total knee replacement.
Metrics: PROMIS: Patient reported Outcomes Measurement Information Systems; RAND short form-36 questionaire Knee Kinematics and Bioelectrical Impedance analysis.
Intervention: LRS (lipedema reduction surgery using Power-assisted liposuction. Preop did mapping of veins and lymphatics with vascular Doppler or Indocyanine green lymphatic mapping
Surgery: Liposuction with Doppler vein mapping, 3/4mm PAL longitudinal cannulas
2019: Canadian Agency for Drugs and Technologies in Health: reviewed clinical effectiveness of liposuction treatment for lipedema from 5 uncontrolled before and after studies in Germany. Severity of lipedema: stage 1-3. Follow up 24-90 months. “All studies suggested that liposuction was effective in reducing extremity size, symptoms of pain and bruising, quality of life, mobility and general impairment.”
Herbst (2021): Survey Outcomes of Lipedema Reduction Surgery in the US, This study used validated questionaires to assess body shape, lower extremity function and a nonvalidated questionnaire for lipedema lifestyle. This was self-reported data by women in the US who had lipedema and underwent lipedema reduction surgery. Patients were Stage1-3 who had at least one lipedema surgery between 2013-2018.
Patient data: 148 women, mostly Stage 2-3, most white and age>50, Over 50% had hypermobile joints. Except for stage 1 pts, average BMI was >30 indicating obesity.
Impact of lipedema reduction surgery: (self-reported with questionnaires):
- Largest area with fatty tissue reduction: proximal leg (44%), knee(37%), ankle (38%),
- Pain: 89% of women reported preop pain; 86% reported pain reduction after lipedema reduction surgery (LRS)
- Swelling: 36% (of 117 women who had preop swelling) stated swelling resolved after LRS, 30% of women were able to stop wearing compression garments within 3 months.
- Bruising: 90% reported bruising preop which decreased to 43%
- Mobility: 81% reported walking was negatively affected by lipedema preop ( 72% knees, 62% thighs, 60% leg pain, 41% knee arthritis) Walking significantly improved: stage 3: 96%, Stage 2: 88%, Stage 1 33%. 82% of women could return to their activities within one month, 11% took 6 weeks.
- Statistically improved in: Walking, quality of life, wt loss and stage reversal.
- Summary: Standard conservative treatment for lipedema reduces tissue fluid but not lipedema tissue. Bariatric surgery not effective for lipedema obesity. “Once standard treatment options have failed to reduce lipedema tissue, LRS becomes the treatment option”. There are no published prospective studies, this study used two validated questionnaires: BSQ-34 and LEFS. Findings: After LRS: reduction in lipedema tissue, reduced stage, improved QOL, reduced pain, perceived benefit from surgery including energy level, strength and ability to walk. 30% of patients were able to stop wearing compression garments within 3 months after LRS
Dadras (2017): Liposuction in the Treatment of Lipedema: A longitudinal Study, 25 women w lipedema followed for min 2 years: significant reduction in spontaneous pain, sensitivity to pressure, feeling of tension, bruising and general impairment. Women also had a significant reduction in need for CDT postop . Used visual analog scale to assess pain and symptoms. Pts BMI ranged from 24.5 to 50 with mean of 35.3. “due to the dev of secondary lymphedema in later stages of disease, liposuction should be implemented as part of the standard therapy for lipedema in the early stage of disease.” This can prevent disease progression, improve QOL and decrease the need for decongestive therapy. Data from this study showed even more benefit in QOL and a larger decrease in need for CDT in Stage 2 vs 3.
Witte (2020) Water-jet-assisted liposuction for the treatment of lipedema:. Standardized treatment protocol for lipo for lipedema estab over 15 years. Prospective study: pre and post questionnaires to assess symptoms and severity. 63 patients, median age 35 BMI: 28.4. Stage 1 or 2 lipedema. Mean F/u for 22 months preop all patients 100% wore compression garments and or lymphatic massage, after only 44% of patients needed any conservative treatment. Mean tissue reduction: 12.9kg This was a study of early stage of disease using only wal. Preop 89% had manual lymphatic massage after: 40%, preop 95% needed compression garments after 59% not needing any.
Kirstein (2020) Patient-Reported Outcomes of Liposuction for Lipedema; Population: 511 patients preop,56 after, 34 filled questionnaire pre and postop; 91.4% pts Stage 2 or 3 ( 62% Stage 3) BMI: 33; ages 18 to 81. Questionnaire: World Health Organization Quality of Life BREF (WHOQOL-BREF) and Patient Health Questionnaire 9 (PHQ-9) Unique features: High percentage of Stage 2 and 3 pts. Meas QOL. Protocol: Mean of 2.38 surgeries, Fat removed/procedure: 3831+/- 1971cc; 57% lower leg only, 23% thigh
Findings: Pain, pressure sensitivity, sensation, heavy leg feeling, limitation in walking, reduction in QOL, extremity appearance all statistically improved. “results demonstrate a beneficial effect on practically every measured aspect of patients’ physical and psychological wellbeing.”
Baumgartner (2020): Improvements in Patients with Lipedema 4,8, and 12 years after liposuction. 60 women followed for up to 12 years. Compared with the results at 8 yrs, results at 12 years showed that improvement persisted with regard to spontaneous pain, sensitivity to pressure, edema, bruising and restriction of movement. Conclusion: The results show, that the positive effects of liposuction last 12 years postoperatively without relevant worsening. They imply that liposuction for lipedema leads to a permanent reduction of symptom severity and need for conservative therapy.
Schlosshauer (2021) Liposuction Treatment improves disease specific quality of life in lipoedema patients. Over 15yrs, 69 patients were treated with liposuction for lipedema and studied retrospectively. The mean age was 50.6 ± 12.8 years, and the average number of liposuction sessions performed was 2.9 ± 1.9, with a mean volume of 1868 ± 885.5 mL of fat removed per side. An additional 20 patients were prospectively evaluated with a Quality of Life questionnaire (Freiburg Life Quality Assessment for lymphatic diseases). Disease-specific quality of life improved on every subscale after liposuction. A higher number of liposuction treatment sessions seem to have a positive effect on general health status in these patients. Conclusion: Liposuction greatly improves the QoL in lipoedema patients
Wollina (2019): Treatment of lipedema by low-volume micro-cannular liposuction in tumescent anesthesia: 111 patients with advanced lipedema were treated with surgical liposuction over 11years. The median age of the patients was 44 years. The median total amount of lipoaspirate was 4,700 ml, with a range of 950-14,250 ml. The median reduction of limb circumference was 6 cm. The median pain level before treatment was 7.8 and 2.2 at the end of the treatment. An improvement of mobility could be achieved in all patients. Liposuction is an effective treatment for painful lipedema.
De Souza (2023): Lymphatic Improvement after suction-assisted lipectomy in a Lipedema Patient.
Case report: 1 patient Country: (Brazil) LRS technique: SAL, removed 3900cc fat aspirate each lower extremity. Follow-up: 9 months Evaluation: limb measurements, lymphoscintigraphy
Impact: 1. LRS resulted in improved lymphatic function. 2. LRS (with compression for 6 months resulted in “improved pain, discomfort and leg heaviness”
This study showed return to normal of lymphatic pathways and drainage after lipedema surgery. In obesity, there is injury, inflammation and lymphatic blockage from fat overgrowth. Lymph system becomes overloaded and cannot accommodate flow.. Excess lymphatic fluid can cause more fat deposition.
References:
- Witte, M Dadras and F.-C. Heck et al., Water-jet-assisted liposuction for the treatment of lipedema: Standardized treatment protocol and results of 63 patients, Journal of Plastic, Reconstructive and Aesthetic Surgery, https://doa.org/10.1016/j.bjps.2020.03.002
- Dadras, P.J. Mallinger, Cord C. Corterier et. Al., Liposuction in the Treatment of Lipedema: A longitudinal Study, Archives of Plastic Surgery, Vol 44/No 4/ July 2017
- J. Stutz, D. Krahl, Water Jet-assisted liposuction for Patients with Lipedema: Histologic and Immnohistologic Analysis of the Aspirates of 30 Lipoedema Patients, Aesthetic Plastic Surgery ,2008 2008DOI:10.1007/s00266-008-9214-y,
- W. Buck, K. Herbst, Lipedema: A Relatively Common Disease with Extremely Common Misconceptions, PRS Global Open, 2016;4:e1043; DOI: 10.1097/GOX.0000000000001043
- -T. Bauer, D. vn Lukowicz et al., New Insights on Lipedema: The enigmatic Disease of the Peripheral Fat, Plastic Reconstructive Surgery 144: 1475, 2019
- Kruppa, I. Georgiou et al., A 10-year Retrospective before and after Study of Lipedema Sugery: Patient-Reported Lipedema-Associated Symptoms Improvement after Multistage Liposuction, Plastic Reconstructive Surgery 149:529e, 2022
- Wright, M. Babula et al., Lipedema Reduction Surgery Improves Pain, Mobility, Physical Function, and Quality of Life: Case Series Report PRS Global Open 2023; 11:e5436; doi: 10.1097/GOX.0000000000005436
- de Souza, R. Vitorasso et al., Lymphatic Improvement after Suction-assisted Lipectomy in a Lipedema Patient, PRS Global Open 2023; 11:e5097; doi: 10.1097/GOX.0000000000005097
- Kruppa, I. Georgiou, et al., Lipedema- pathogenesis, diagnosis and treatment options; Dtsch Arztebl Int 2020; 117: 396-403. DOI: 10.3238/arztebl.2020.0396
- Herbst, L. A. Kahn et al., Standard of Care for lipedema in the United States, Phlebology Vol 36, No 10, December 2021, pp 779-796, doi.org.10.1177/02683555211015887
- Herbst, E.A.Hansen et al., Survery Outcomes of Lipedema Reduction Surgery in the United States, Plastic Reconstructive Surgery Global Open 2021;9:e3553; doi: 10.1097/GOX.0000000000003553
- Kirstein, M. Hamatschek, et al., Patient-Reported Outcomes of Liposuciton for Lipedema Treatment Healthcare 2023, 11, 2020. Doi.org/10.3390/healthcare11142020
- Podda, M. Kovacs et al., A randomized controlled multicentre investigator-blinded clinical trial comparing efficacy and safety of surgery versus complex physical decongestive therapy for Lipedema (LIPLEG) Trials (2021) 22.758
- Baumgartner, M. Hueppe, et al., Improvements in Patients with Lipedema 4,8, and 12 years after liposuction, Phlebology, 2021 Mar;36(2):152-159. doi: 10.1177/0268355520949775
- Schlosshauer, C. Heiss et al. Liposuction Treatment improves disease specific quality of life in lipoedema patietns, Int Wound J, 2021 Dec;18(6):923-931. doi: 10.1111/iwj.13608
- Wollina,K. Heinig. Treatment of lipedema by low-volume micro-cannular liposuction in tumescent anesthesia: Results in 111 patients, Dermatol Ther . 2019 Mar;32(2):e12820. doi: 10.1111/dth.12820.
III:^ Insurance Guidelines for surgical treatment of lipedema (BCBS) with comment (red):
- “primary focus of treatment is weight normalization (if coexisting obesity is present), exercise and decongestive therapy. Liposuction has been proposed as a surgical treatment option for lipedema”
Lipedema is not a form of obesity. Weight reduction strategies can lower total weight but will not reduce lipedema fat. Weight loss is most helpful in reducing complications from surgery. It is often impossible to achieve weight “normalization” with lipedema. Exercise is often restricted because of heaviness of legs and impaired mobility. Aquatic exercise can be beneficial. Decongestive therapy can be helpful in reducing inflammatory fluid temporarily but does not address the root problem: the lipedema fat. Liposuction has been shown in 9 peer-reviewed studies to have significant benefit in reducing pain, disability, increasing mobility and slowing progression of disease. These studies have used validated measures of patient care and symptom reporting.
- Insurance criteria for “coverage” of surgical treatment of lipedema:
- Diagnosis of lipedema made to include ALL the following clinical findings:
- Bilateral symmetrical fat deposition, disproportionally affecting limbs and sparing the hands and feet
- History of easy bruising or bruising without apparent cause in lipedema affected areas Yes, this is a hallmark sign of lipedema. Surgical treatment early in stage 1,2 can correct this sign.
- Diagnosis of lipedema made to include ALL the following clinical findings:
- Pain and or hypersensitivity to touch in lipedema affected areas Yes, most all women (80%) present with pain or pressure-sensitivity in lipedema areas. But pain is not present in all women with lipedema.
- Significant physical impairment: difficulty ambulating or performing activities of daily living or medical complications such as recurrent cellulitis or skin ulceration. These clinical findings are present in late stage disease or with lipolipedema. Data shows that early intervention with surgery has the best results in all functional evaluations: increase mobility, increase quality of life, continue to work, less or eliminate pain, swelling, disability.
- Lack of effective weight loss measures as documented in the medical records through nutrition and medical interventions and clinic visits over 6 consecutive months. Weight loss measures for obesity are not effective in reducing lipedema. This has been clinically proven. Making patients wait 6 months delays early surgical intervention.
- No response to at least 3 consecutive months of conservative management including medical grade compression garments, complex decongestive lymphatic therapy and sequential pneumatic compression. This is reasonable if the patient can afford and apply compression garments. Patients very sensitive to pressure and women with large lipedema of the thighs cannot wear garments. Decongestive lymphatic treatments are expensive ($150-200 per session). Lymph-press and pneumatic compression devices are self-pay.
- No pitting edema. This is a feature of congestive failure not lipedema, agree.
- Surgery by hospital credentialled board-certified plastic surgeon.
- Evidence assessment: ( review of existing literature, reviewed 8/23)
- “body of evidence for treatment of lipedema using liposuction is limited to a small number of single arms studies on patient subjective self-assessment using clinical scales not validated for lipedema. There are now 9 peer-reviewed studies with validated questionaires and statistical analysis from the US and Germany showing the unequivocal benefit of early surgical intervention for lipedema treatment. Yes, single arm studies is the only ethicak way to collect data for these patients. These studies used pre and post questionaires and clinical measurements ( Wright). Because lipedema is a relatively new diagnosis, questionaires were used having been validated by agencies like WHO.
- All studies reviewed suggested that liposuction was effective in reducing extremity size, symptoms of pain and bruising, quality of life, mobility and general impairment. This is the consistent conclusion. Surgery does increase mobility, increases function, less diability.
- But the conclusion was: studies were non-randomized, small, heterogeneous and at high risk for bias. All used measures not validated for lipedema. Therefore “reliability of reported outcomes is uncertain and durability of the procedure is unknown. The evidence is based mainly on expert opinion.” This is the flaw: there are two treatment options for lipedema: conservative decompressive therapy ( garments, manual lymphatic drainage, lymph-press) and surgery. The treatments are not equivalent, they are complimentary. Therefore a randomized study is not ethical. The statement that “reliability of reported outcomes is uncertain” is just not true. All studies showed significant functional benefit. Also surgery was shown to slow progression of disease for up to 12 years.
- The standard of care guidelines was published by a US committee of lipedema experts which included therapeutic recommendation for use of liposuction in patients who have failed conservative measures. “ Insurance guidelines does not support consensus committee findings.” These expert guidelines were written by US Lipedema experts. This group is in the best place to provide guidance for patients and for doctors treating these patients. Why does insurance not support the expert consensus opinion?
IV: Appendix 1: Lipedema Diagnosis:
- Diagnosis is made clinically, excluding obesity and lymphedema
- Abnormal disproportionate fat growth in the extremities in women
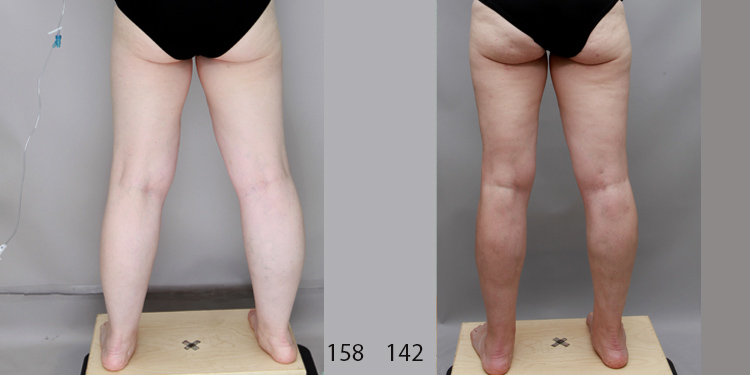
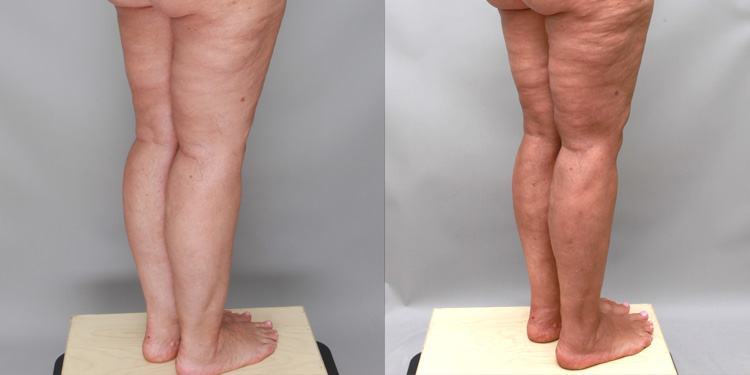
- Cuff sign: a sharp demarcation at the ankle
- Abnormal fat is sensitive to pressure, painful, can have easy bruising
- Fat deposits do not respond to normal weight loss.
- Abnormal disproportionate fat growth in the extremities in women
- Stages reflect the extent of disease:
- Stage 1:
- skin is smooth; under skin: small nodules
- Stage 2:
- Skin may be uneven or wavy, may have indentation
- Under skin: palpable nodules ( walnut size nodules)
- Stage 3:
- Skin: thick or hard feeling to skin, divots or folds
- Under skin: disfiguring larger fat deposits
- Progressive disease can be accompanied by:
- Osteoarthritis, esp of the knee joint
- Reduced mobility or ambulation
- Stage 1:
- Psychosocial impairment or reduced self-esteem
- Stage 4: lymphedema
- Types: ( disease patterns)
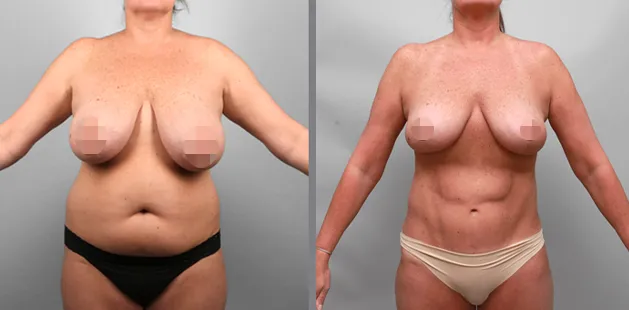
- Type 1: Pelvis: buttocks
- Type 2: Pelvis and thighs and knees ( can include buttocks)
- Type 3: Pelvis, thighs, knees and legs to ankles
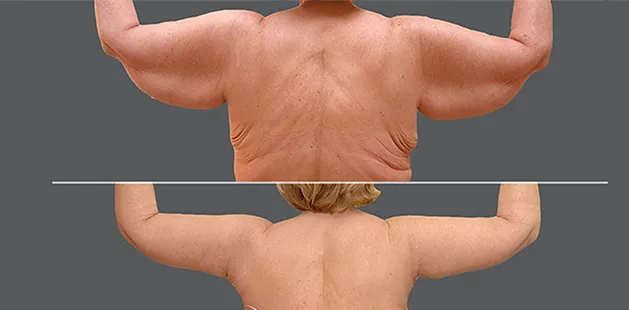
- Type 4: Arms, can extend below elbow not involving hands
- Type 5: Legs
- Common presentations:
- Type2 and 4: Arms and Pelvis, thighs and knees
- Type 3 and 4: Arms and Pelvis thighs, knees, legs